
Saturday, 11 August 2012
Initial detection of CKD Algorithm
Algorithm for management of hypertension in people with CKD

ABCD2 Stroke and TIA Risk Assessment

Thursday, 9 August 2012
Algorithm for management of persistent microscopic haematuria

Monday, 6 August 2012
Diagnosis, assessment and initial management of Diabetes
From Diabetes Management in General Practice 2011/2012 (Diabetes Australia)


 What to recommend to a new diabetic:
What to recommend to a new diabetic:
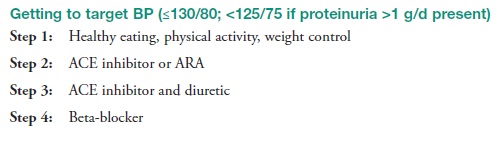
 I tend to use Telmisartan ie Micardis, due to its excellent tolerability as well as positive effects on cholesterol, microalbuminuria and proteinuria, and reduced risk of myocardial infarctions, strokes and death from cardiovascular events. However, fosinopril ie Monopril is also a good option because there is no need to reduce the dose in renal impairment, but it does commonly cause in irritating cough
I tend to use Telmisartan ie Micardis, due to its excellent tolerability as well as positive effects on cholesterol, microalbuminuria and proteinuria, and reduced risk of myocardial infarctions, strokes and death from cardiovascular events. However, fosinopril ie Monopril is also a good option because there is no need to reduce the dose in renal impairment, but it does commonly cause in irritating cough




- Diet & Exercise - trial for 6 weeks (decrease saturated fats, eat small portions, change to low GI foods, exercise minimum 30mins 5 days per week). If unsuccessful, then...
- Medications -
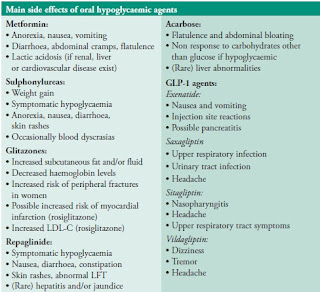
- Oral hypoglycaemic agents. My my current favorites to use are metformin extended release, GLP-1 agonist ie Exenatide and DPP4 inhibitors ie Januvia or Galvus. Sulphonyureas is often used as a 2nd line agent after metformin but a local endocrinologist has advised that perhaps exenatide should be the next step due to lack of hypoglycaemic episodes as well as weight loss. Acarbose is also a very good agent but poorly tolerated due to excess bloating and flatulence.
- Insulin. Lantus, Mixtard, Actrapid are my go-to insulins. Remember to also prescribe Glucagen Hypo Kit - 1 at work and 1 at home.

- Antihypertensives
- Cholesterol
Hypercholesteraemia: Statins ie lipitor or crestor. If not tolerable or need stronger control add exetimibe (Ezetrol), then resins such as cholestyramine (Questran) or colestipol (colestig) for hypercholesteraemia
Hypertriglyceridaemia: Fibrates such as fenofibrate (Lipidil) or gemfibrozil (lopid).

- 100mg Aspirin if no contraindication
Referrals
- Diabetic educator - initially, then as needed
- Dietitian - initially, then as needed
- Podiatry - if issues with feet, or need help to cut toenails. Also worth getting it checked initially for potential problem areas
- Optometry/ophthalmology at least every 2 years
- Dentist - once to twice yearly checkup
- Renal physician - consider if getting proteinuria
- Endocrinologist - if sugars are difficult to control or significant complications, pregnancy, gestational diabetes, children/adolescents/adults with type 1 diabetes




Flowchart for TFTs - for GPs
 A nice summary of TFT interpretation - based on UK guidelines. Click above link for original website.
A nice summary of TFT interpretation - based on UK guidelines. Click above link for original website.

Thyroid nodule - Workup

Follow up of benign thyroid nodules:
- a) all benign thyroid nodules should be followed with serial US examinations 6–18 months after the initial FNA. If nodule size is stable (i.e., no more than a 50% change in volume or <20% increase in at least two nodule dimensions in solid nodules or in the solid portion of mixed cystic–solid nodules), the interval before the next follow-up clinical examination or US may be longer, e.g., every 3–5 years.
- (b) If there is evidence for nodule growth either by palpation or sonographically (more than a 50% change in volume or a 20% increase in at least two nodule dimensions with a minimal increase of 2 mm in solid nodules or in the solid portion of mixed cystic–solid nodules), the FNA should be repeated, preferably with US guidance.
.

Subscribe to:
Comments (Atom)